Background: According to EU Regulation 2024/1849 (June 13, 2024; published in the Official Journal on July 10, 2024), the use of dental amalgam in the European Union is largely prohibited starting January 1, 2025, due to environmental and health concerns.
Key Points:
The use of dental amalgam is now heavily restricted, especially for children, pregnant women, and breastfeeding mothers.
This measure is part of a broader environmental initiative aimed at reducing mercury exposure.
While the amount of mercury released from amalgam fillings is considered safe for health, their use is declining and being replaced by alternative materials such as composite resins and glass ionomer cements.
Existing Amalgam Fillings:
No need to replace intact fillings.
Studies show that a well-maintained amalgam filling can last for many years with good oral hygiene and regular dental check-ups.
A filling only needs to be replaced if it is damaged, shows cracks, or has secondary caries.
But how can I tell if my amalgam fillings are still intact?
Take the Self-test
To assess the condition of your filling, you can use the following comparative images as a guide.
IMPORTANT: Only your dentist can make a reliable diagnosis.
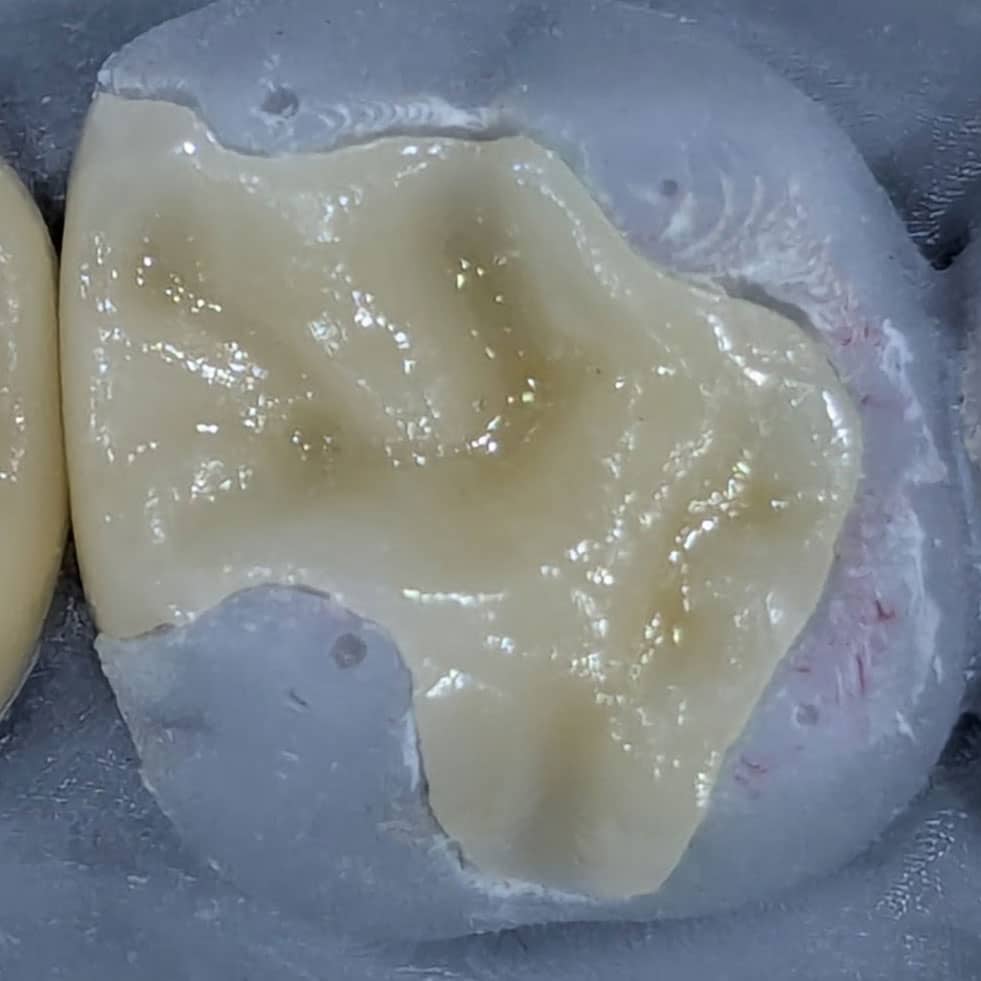
Intact Filling
A perfect filling has a clean, tight seal with the tooth. There are no visible gaps or discolorations along the edges.
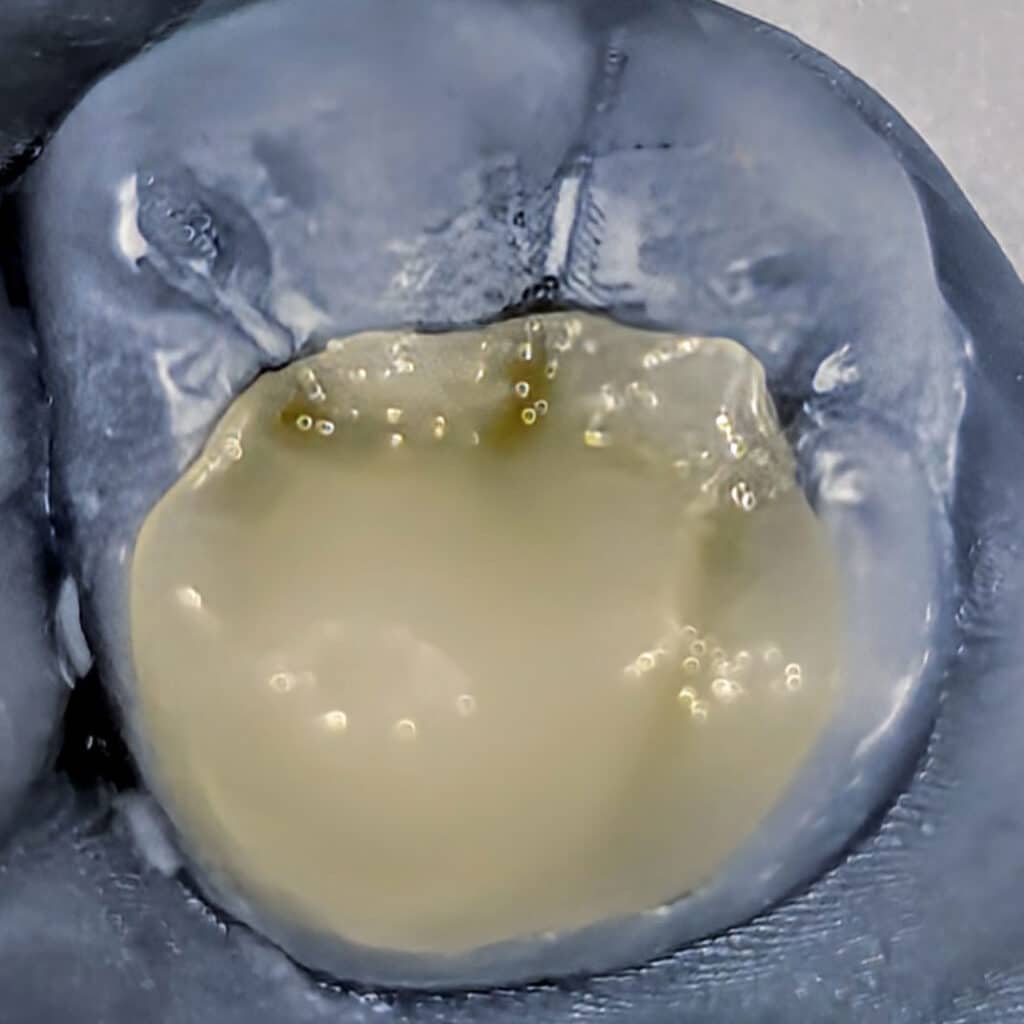
Margin Gap
A margin gap is a leakage between the filling and the tooth. This allows bacteria to enter and cause decay, often without producing any immediate pain.
Crack
Cracks can form either in the amalgam itself or in the surrounding tooth structure. Hairline cracks in the enamel are an early sign of instability and may lead to fracture.
Fracture
A fracture is an obvious weak point where the filling or parts of the tooth have broken off. This can affect chewing function and make the tooth more vulnerable to further damage.
Sec. Caries
Secondary caries is decay that develops underneath an existing filling. It is often not directly visible and is usually only detected on an X-ray as a dark area beneath the filling.
Ceramic instead of Amalgam state-of-the-art 3D technology for your dental health
If a replacement becomes necessary, various modern materials are available. Ceramic restorations (inlays, onlays, overlays, or partial crowns) are considered by research to be the highest-quality option.
Inlay
Onlay
Overlay
Partial Crown
At our practice, we consciously choose high-quality ceramic as a sustainable alternative to amalgam. Ceramic fillings and inlays are not only biocompatible and metal-free, but also impress with their natural tooth color and excellent compatibility.
Perfect Aesthetics and Natural Transparency
Ceramic matches the color of your natural teeth perfectly and is barely distinguishable from your own tooth structure.
Biocompatibility
Ceramic is metal- and mercury-free, making it an ideal choice for people with allergies.
Maximum Strength and Longevity
Studies show that ceramic restorations, with proper care, can last over 30 years.
Maximum Tooth Preservation
With adhesive techniques, as little healthy tooth structure as possible is removed during preparation.
Thanks to state-of-the-art 3D technology, we can precisely plan ceramic restorations and customize them for you—often within a single appointment. The digital process enables maximum accuracy of fit, durability, and an aesthetically perfect solution that blends harmoniously with your natural teeth.
This is how we combine dentistry with innovation:metal-free, gentle, and state-of-the-art—for a healthy and beautiful smile.
THe History of Amalgam:
What exactly is Amalgam?
A metal alloy consisting mainly of mercury (approx. 50%).
Other components: silver, tin, copper, and sometimes zinc.
Amalgam is placed in the tooth in a plastic state and hardens there—stable, durable, and inexpensive.
Historical milestones:
Ancient beginnings: There are references to mercury-containing filling materials as early as ancient China (approx. 600 AD).
16th century: The first descriptions of mercury-containing dental fillings appear in Europe.
19th century:
1819: Berlin physician Auguste Taveau experiments with a mixture of silver, tin, and mercury.
1830s: Amalgam arrives in America and Europe – quickly becoming popular, but also controversial.
“Amalgam war”: Dentists and doctors argue about the possible health risks of mercury. Some professional associations temporarily ban amalgam.
20th century:
Amalgam establishes itself worldwide as the standard filling material: inexpensive, easy to work with, very durable.
Particularly widespread in the post-war period, as alternatives were more expensive or less stable.
Late 20th century to present day:
Growing criticism due to possible mercury contamination.
New materials such as composites (plastic fillings) and ceramics are becoming more widespread.
2018: The EU restricts the use of amalgam (e.g., no longer for children under 15 or pregnant women).
Many countries are planning a gradual phase-out by 2030.
HEALTH INSURANCE ALTERNATIVES: STANDARD CARE provided by statutory health insurance
Front teeth: Adhesive composite fillings
Back teeth: Direct restorations using self-adhesive materials (e.g., glass ionomer cements, self-adhesive composite hybrids)
Bulk fill composites if medically necessary, if self-adhesive materials are not sufficient for large cavities
What does this mean for YOU?
A durability of only a few years means that the filling will probably have to be replaced several times. When the old filling is removed, a piece of healthy tooth substance is always lost. Over time, this can make the tooth smaller, more sensitive, or even brittle. It also increases the risk of renewed caries or the need for root canal treatment. The frequency of visits to the dentist also plays a role: those who need new fillings regularly have to visit the dentist more often and invest more time and money. That is why it is important to use durable materials and practice careful dental care.
Why don’t health insurance companies reimburse high-quality care?
Statutory health insurance is bound by the principle of economic efficiency and only covers what is “sufficient, economical, and appropriate” and does not “exceed what is necessary.” This means that state-of-the-art treatment based on the latest scientific findings is not covered. However, the amount regulated by law is offset.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.